Sometimes fungal hyphae or other structures, such as spherules, are directly visible, but scanty hyphae and small yeasts are easilSometimes fungal hyphae or other structures, such as spherules, are directly visible, but scanty hyphae and small yeasts are easily missed.
The host response to fungi is varied, partly depending on whether the patient is immunocompetent or immunocompromised. No host cell reaction may be seen in immunocompromised patients, especially with pulmonary Pneumocystis and disseminated Cryptococcus infections. Some important host responses that are visible on histopathology include:
- Mixed granulomatous reaction, seen with both yeast and filamentous fungal infection.
- Granulomas with caseous necrosis, mimicking mycobacterial infections seen with Histoplasma and Coccidioides infections.
- Vascular invasion and secondary thrombosis with infarction and haemorrhage, seen especially in neutropenic patients with Aspergillus or Mucorales infection.
- Epithelial hyperplasia of skin with mixed inflammation and abscesses within the epidermis, seen with cutaneous fungal infection.
The British Society for Medical Mycology has published standards of good practice for pathologists when a fungal infection is suspected or confirmed (Schelenz et al, 2015). The need for processing tissue rapidly and reporting by telephone is paramount. These are the summary recommendations:
Specialised stains
Specialised stains should be done in parallel with standard stains if mycosis or another infection is to be assessed or excluded:
• Standard stain: haematoxylin and eosin (H&E) on histopathology slides; Giemsa or Papanicolaou on smears
• Triple set of stains: Ziehl–Neelsen stain for acid-fast organisms; Gram stain for bacteria, fungi, and others; Grocott silver stain, or periodic acid–Schiff, to highlight fungi
Reporting of results
Report fungal morphology (yeast or hyphae), including the following:
• Whether a yeast is small, medium, or large
• Whether a yeast has cross walls or septa (ie, is splitting rather than budding)
• Whether a hyphal form has usual width, or has a dilated, bizarre shape
• Whether H&E-stained fungi are pigmented and brown, or are unpigmented and colourless or pale blue. Positive results should be telephoned to clinicians immediately.
For an excellent overview of the special fungal stains and the appearance of most common fungi, please visit Doctor Fungus

For more detailed information please see the review by Guarner & Brandt (2011)
Teaching slides and videos
Watch our playlist below, or access the YouTube channels of Jerad Gardner and WashingtonDeceit for clear explanations of the histological appearances of the major fungal pathogens in different organs.
Or find slide images on #PathTwitter

Courses
Special fungal stains
On hematoxylin and eosin (H&E), all fungi show pink cytoplasm, blue nuclei and no colouration of the wall.
Tissue Gram stains can colour Candida spp. blue, consistent with a Gram-positive organism. With an acid-fast stain for Mycobacteria, Blastomyces and Histoplasma can be appear red and be acid-fast staining.
Standard histological stains for fungi are Grocott (methanmine) silver (GMS) stain or Periodic acid-Schiff (PAS). The GMS stain is more sensitive than the PAS stain, but has a signal to noise issue, whereby it stains inflammatory cells (lysosomes) and tissue reticulin, in addition to fungi. PAS staining has the slight advantage in that the morphology of the tissue adjacent to the fungi can be better visualised, but this can be addressed using a GMS stain and H&E counterstain. Inclusion of good control sections is mandatory, as some fungi such as Mucorales may require longer staining times and other fungi can be ‘over-stained’.
Guidelines
Demonstration of fungi in tissue is confirmatory of fungal infection. So the 2008 European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium (EORTC/MSGERC) definitions of invasive fungal infection carry these statements for proven infections:
- Moulds: Histopathologic, cytopathologic, or direct microscopic examination of a specimen obtained by needle aspiration or biopsy in which hyphae or melanized yeast-like forms are seen accompanied by evidence of associated tissue damage.
- Yeasts: Histopathologic, cytopathologic, or direct microscopic examination of a specimen obtained by needle aspiration or biopsy from a normally sterile site (other than mucous membranes) showing yeast cells—for example, Cryptococcus species indicated by encapsulated budding yeasts or Candida species showing pseudohyphae or true hyphae.
PARALLEL PROCESSING: The British Society for Medical Mycology Standards of Care (2015) set out 2 standards for histopathology:
“All tissues from immunocompromised (including corticosteroid-treated) patients and those with suspected fungal infection should be stained with fungal stains such as PAS, silver, or fluorescent stains, in parallel with regular stains. Speed is critically important in achieving an early diagnosis, and the practice of assessing H&E stains of tissues before deciding whether to use specialised stains for fungi frequently introduces fatal delays for patients. Clear indication on all pathology request cards that the patient is immunocompromised is critically important.”
BSMM Standards of Care (2003)
STANDARD STAINS: Standard histological stains for fungi are GMS stain or PAS. The GMS stain is more sensitive than the PAS stain, but has a signal to noise issue in that it stains inflammatory cells (lysosomes) and tissue reticulin, in addition to fungi. PAS staining has the slight advantage that the morphology of the tissue adjacent to the fungi can be better visualised, but this can be addressed using a GMS stain and H&E counter-stain. Inclusion of good control sections is mandatory as some fungi such as Mucorales may require longer staining times and other fungi can be ‘over-stained’.
On H&E, all fungi show pink cytoplasm, blue nuclei and no colouration of the wall. Tissue Gram stains can stain Candida spp. blue, consistent with a Gram positive organism. With an acid-fast stain for Mycobacterium, Blastomyces and Histoplasma can be appear red and be acid-fast staining.
Diagnosis
Some fungi are distinctive enough on histopathology that a definitive aetiological diagnosis can be made.
Table 1
| Species | Appearance | Tissue reaction |
| Cryptococcus | Narrow-based budding yeasts (4–10 µm) with a thick capsule | None or granulomatous reaction, occasionally fibrosis |
| Blastomyces dermatitidis | Broad-based budding yeasts (10–15 µm) | Mixed suppurative and granulomatous inflammation typical |
| Histoplasma capsulatum | Small yeasts (2–4 µm) clustered inside macrophages with narrow-based budding | Several appearances depending on chronicity of infection; vascular necrosis and granulomatous inflammation |
| Penicillium marneffei | Small oval yeasts (2–5 µm) with a transverse septum, indicating division by fission | Mixed suppurative and granulomatous inflammation or necrosis with little reaction |
| Sporothrix schenckii | Round, oval, or cigar-shaped yeasts (2-6+µm) with narrow-based or tube-like budding | Mixed suppurative (including eosinophils) and granulomatous inflammation, Hoeppli-Splendore phenomenon frequent |
| Coccidioides immitis/posadasii | Spherules (10-100 µm) with multiple endospores (2-5 µm), (often confused with yeasts) | Mixed suppurative (including eosinophils) and granulomatous inflammation with a rim of lymphocytes, Hoeppli-Splendore phenomenon likely |
| Paracoccidioides brasiliensis | Spherical large yeasts (4-60 µm) surrounded by multiple buds [ship’s wheel] with an optically clear space between the fungus and surrounding tissue | Yeasts are usually found inside multinucleated giant cells. Mixed suppurative and granulomatous inflammation surrounded by fibrosis |
Immunohistochemistry (IHC)
Immunohistochemistry (IHC) or immunocytochemistry is a method for localising specific antigens in tissues or cells, based on antigen-antibodies recognition. Specificity should derive from binding of an antibody with its counterpart antigen at a light microscopic level. The use of an enzymatic label antibody such as horseradish peroxidase allows visualisation of the labeled antibody using conventional light microscopy in the presence of a suitable chromogenic substrate system.
IHC is now applied to routinely formalin-fixed, paraffin-embedded tissue sections. Depending on the colorimetric developer, fungi stain dark brown or red, usually with a counterstain of hematoxylin. Immunohistochemical methods have the potential advantage of providing a rapid and specific identification of several fungi, allowing pathologists to identify unusual filamentous and yeast-like infections and accurately distinguish them from confounding artefacts.
IHC for Candida, Aspergillus, Blastomyces, Cryptococcus, Histoplasma, Coccidioides, Pneumocystis, Sporothrix, Paracoccidioides, Penicillium and Mucorales have been developed and some are available commercially. For the identification of Aspergillus species, polyclonal and monoclonal antibodies have been produced but most of these antibodies cross-react with other fungi. Cross-reactivity of the antibodies is a common problem limiting their use.
In situ hybridisation (ISH)
In situ hybridization (ISH) uses molecular probes for different fungi to contribute to identification. Most probes are ribosomal to amplify the tissue signal. Depending on the colorimetric developer, fungi stain dark brown or red. Probes published in the literature include those for Candida, Aspergillus, Blastomyces, Cryptococcus, Histoplasma, Coccidioides, Pneumocystis, Sporothrix, Mucorales, Fusarium and Pseudallescheria.
The accuracy of ISH appears to be high, but sensitivity on formalin-fixed tissue is reduced.
Identification of fungi in tissue
Fungal DNA can be amplified directly from tissue (preferably fresh), using broad-range polymerase chain reaction (PCR) assays targeting ribosomal ribonucleic acid (RNA) genes, especially the internal transcribed spacer (ITS) 1 or ITS 2 regions, or 18S or 28S. DNA extraction and PCR methods are published allowing amplification of DNA from many diverse fungi in the presence of human DNA. The PCR product can then be sequenced and sequences compared with the publically available databases. This allows direct identification, although DNA extraction and amplification fails in up to 50% of cases from formalin-fixed tissue.
Reporting results
The first key requirement of histopathological reporting is confidence that a fungal infection is or is not present in the tissue sample. Compared with culture or other diagnostic testing, the sensitivity of histology is at best 80% (and often as low as 20%, especially if specialised GMS or PAS stains are not done). However, negative reports are valuable, despite the less than perfect sensitivity, as some cultures and antigen tests are falsely positive. Diagnosing a fungal infection, as opposed to malignancy, tuberculosis, leishmaniasis or auto-immune disorder (to name some differential diagnoses) has major implications for each patient.
Histopathologists should report both the fungal morphology and the tissue reaction, ie, what they see in the tissue. The histological reaction often determines the precise diagnosis, such as granulomatous fungal rhinosinusitis. Histopathologists should describe whether the fungal morphology is yeast or hyphal (or both as in dimorphic infection) and the yeast or hyphal diameter. They should note the type of budding of the yeast – narrow or broad-based, or fission. For hyphae, they should note whether the hyphal form is regularly septated or not, are the hyphae the usual width of Aspergillus hyphae (3-12 um) or wider, branching angle or have a dilated, bizarre shape, more consistent with Mucorales. They should also note if any surrounding brown pigmentation is present (dematicaeous) or are unpigmented colourless/pale blue on H&E stain (hyaline). An excellent resource was published by Guarner & Brandt (2011).
Some fungi are highly distinctive and what is seen is sufficient to make a definitive aetiological (fungal) diagnosis (see Table 1). Others are less so, in particular filamentous fungi. The number of species involved is large, although Aspergillus fumigatus remains the most common mould infection worldwide. Candida spp., with the common exception of C. glabrata, are dimorphic, so that both yeast cells and hyphae are visualised together. In heavily immunocompromised patients, mixed infections are now seen in up to 20% of patients, further complicating interpretation of positive findings. A few key distinctions are important for immediate treatment decisions, notably:
- Distinguishing the characteristic Mucorales hyphae from other hyphae, as all Mucorales are resistant to fluconazole, itraconazole, voriconazole and echinocandin antifungals.
- Identifying Pneumocystis jirovecii, which is generally azole, amphotericin B and echinocandin resistant.
- Distinguishing the small yeasts without hyphae, characteristic of Candida glabrata, which is fluconazole resistant.
- Distinguishing Cryptococcus spp. from Candida spp, as Cryptococcus spp. are echinocandin resistant.
PAS stain: disseminated Trichosporon spp. infection x60. The PAS stain shows the tissue morphology, with bright pink yeasts also visible 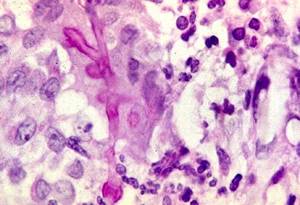
PAS stain: patient with chronic granulomatous disease showing a 45 degree branching hypha within a giant cell. Rather bulbous hyphal ends are also seem, which is sometimes found in Aspergillus spp. infections, histologically (x800) 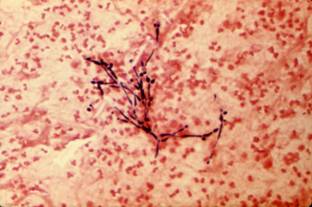
Gram stain. Candida albicans in a section of lung, confirming an invasive Candida pneumonia. Both yeasts and hyphae are visible. Candida is staining Gram positive. 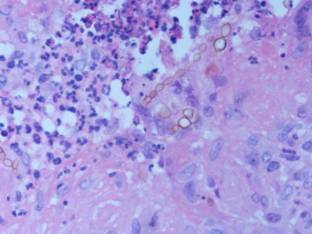
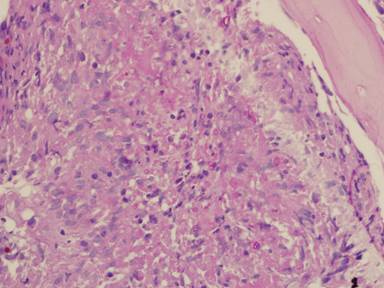
H&E stain. An example of dematiacous fungi causing chromoblastomycosis. Strings of fungal cells, of 2 different sizes, with brown melanin on the fungal cell surface (x600) 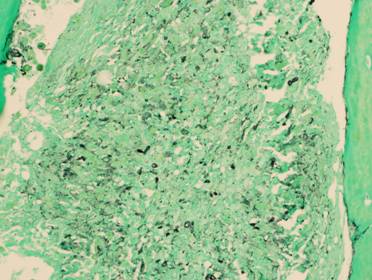
GMS stain: disseminated Trichosporon spp. infection x60. Substantial background staining of elastin is seen, with more prominent yeasts superimposed